Last updated on May 28th, 2024 at 12:19 pm
Learn all about the truth about babywearing, sponsored by our friends at Boppy, creators of the Boppy ComfyFit Baby Carrier.

Wear your baby in confidence when out and about with the easy, comfy and supportive Boppy® ComfyFit® Baby Carrier. This is a great carrier if you’re looking for a hybrid of structure and wrap. It’s easy and quick to put on while also being lightweight and soft.
The Boppy® ComfyFit® Baby Carrier is designed for babies between 8-35 lbs. (3,5-15 kg) with the option to front-face in or out.
- The easiest way to wear your baby—simply click, strap, tie and go
- Made of soft fabric with spandex, which makes it comfy just like yoga apparel
- Lightweight, hybrid carrier with a structured seat for a secure position

Pick from three great color options: black, grey, or navy blue. All colors feature:
- Zippered pocket in waist belt to keep small items conveniently in reach
- Stash n’ Go Pouch makes your carrier small and portable when not in use
- Machine washable for easy care, because little messes happen
- Simple to share between caregivers; one size fits most
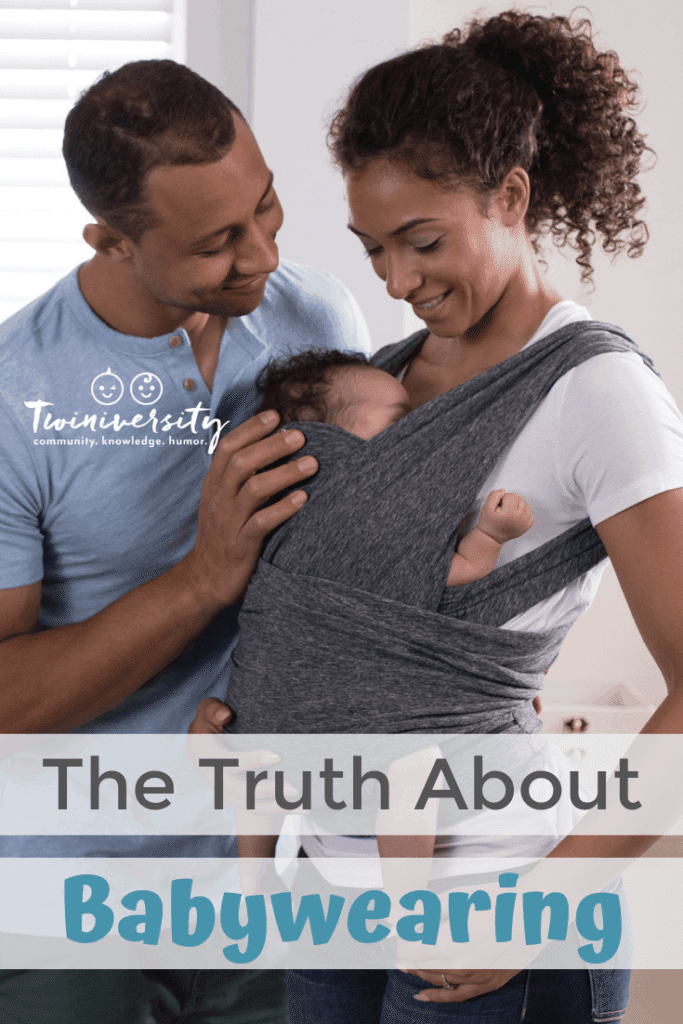
Babywearing is the practice of wearing an infant or toddler using a sling or carrier. It has been practiced worldwide for centuries. Even with a long history, many caregivers are hesitant to try wearing due to fears that it could potentially lead to harm of the child. This article is dedicated to easing fears that prevent caregivers from taking advantage of these products and the freedom to move they provide.
Myth: Babywearing Will Cause Hip Dysplasia
Fact:
The treatment for hip dysplasia is increasing the time the baby or toddler spends with the femur (upper leg bone) in the acetabulum (hip socket). This position is with the legs abducted (spread apart) and the hip flexed (bent). Carriers that promote this position are actually safe for all ages. It would be suggested that any position promoting legs straight, hip extension (legs behind hips) and adducted (together) be avoided for extended periods of time.

Myth: Babywearing Is Unsafe
Fact: There Are Tips to Ensure Safety of the Child
- First: Ensure the baby is able to breathe well. This is best in an upright position. Wear the baby high enough on you that you are able to monitor breathing and ensure that the chin is off the chest. A position where the chin is on the chest naturally closes the airway. This is most important for infants that lack head control and are unable to communicate distress.
- Second: Practice using all carriers and positions with a spotter present. This will ensure the wearer’s and the child’s safety. At very least be sure to practice near soft surfaces until the wearer is comfortable with the different carrying positions and placing the child or children in the carrying device.
- Third: Prior to use, inspect the carrier. Over time there is wear and tear. Ensure the stitching is secure and there does not appear to be any weak spots in the fabric. Always read the label before purchasing to ensure quality, baby-safe materials.
- Finally, if you are uncomfortable with wearing, there are babywearing instructors across the nation available for consultation.

Myth: Baby Will Develop ADD
Fact:
There have been no controlled trials or case studies relating babywearing to the development of ADD. The limited research available in regards to babywearing states babies worn for 3 hours a day cried less than counterparts that were not worn. Additionally, the caregiver wearing the baby consistently is more attune to the child’s different facial expressions and movements, which allowed for decreased guessing as to the child’s current need. The more confident the caregiver becomes in reading the infant, the more secure the child is in return. A bond is established and the infant knows its needs will be met.
Myth: Babies Should Not Face Out
Fact:
Parents holding a child in his/her arms facing forward tend to tire after 15 minutes and the baby’s position is naturally changed due to fatigue. Babywearing instructor Laura McCarthy, MSW, LSW, does not discourage her clients from using forward-facing holds as long as the child has excellent head control before the position is attempted. Then the wearer should be aware of the amount of time the child has been facing forward and use the natural limit as a guide for this position. When using a carrier, the parent may not tire as quickly but it is important to remember the infant may tire first. Therefore Laura advises looking for distress signs and adjusting the hold position appropriately. It is also important to note the child should be awake in this position because the infant or toddler needs to be able to demonstrate head control.

Myth: Twin Babywearing Is Not Possible
Fact:
There are multiple products on the market that are safe for the wearer and the infants. It is important to research each product. Using the aforementioned safety precautions: upright, hips abducted and flexed and baby’s chin off his/her chest, it is possible for a caregiver to safely carry both children. This being said the caregiver should be aware of his or her fatigue. When the wearer is becoming tired it is time to stop wearing the children so all participants are safe.
Take Home Message
The age-old practice of babywearing frees up the caregiver’s arms to perform tasks around the home and in the community while still being attentive to the infant. This practice decreases crying while increasing the caregiver’s ability to determine the baby’s expressed needs. Wearing a child with correct body mechanics, for the wearer and the child, is safe and beneficial for all involved.
By Maryjean Starr, SPT and Carolyn Wincer PT, DPT, CLT-LANA, OCS
Maryjean Starr is currently in her final year of the Doctor of Physical Therapy program at the University of Pittsburgh. Specialty interest in physical therapy includes manual orthopedic, sports, lymphedema, and pelvic floor therapy. Hobbies include running, swimming, biking, hiking and reading.
Carolyn R. Wincer, PT, DPT, CLT-LANA, OCS, is married with a four-year-old daughter and twin toddler boys. She has been a physical therapist for ten years and is the facility director of a physical therapy clinic. The letters after her name mean: DPT = doctorate of physical therapy, CLT-LANA = certified lymphedema therapist, OCS = board certified in orthopedics.